Introduction
Due to its contact nature, football is one of the sports with the highest incidence rates [1]. According to various authors, football holds a leading position in injury frequency among team sports, such as baseball, American football, and basketball [2]. This metric depends on the training level of the athletes and coaching staff, the equipment and resources of the training process, training workload intensity, the use of specialized warm-up programs, and other factors [1–5]. At the same time, the injury incidence among young athletes is quite high, which can result in a player being sidelined from the training and match process for an extended period [1–3]. Therefore, a timely analysis of the causes and structure of injuries is crucial for the subsequent development of preventive measures and injury reduction strategies.
Study Objective — to evaluate the incidence rate and patterns of injuries in amateur football players aged 15–17.
Study Objectives:
- To evaluate the incidence rate in amateur football players aged 15–17 during the training and match process.
- To evaluate the injury patterns in amateur football players aged 15–17 during the training and match process based on anatomical location and injury severity.
- To compare the incidence and patterns of training-related and match-related injuries.
Study Design
A retrospective cohort study was conducted among adolescent boys aged 15–17 years playing amateur football in the «Troparevo» regional football league in Moscow. The study was carried out during the training and competitive periods from September to December 2025.
Materials and Methods
The study included 14 amateur football players aged 15–17 years. Over a 4-month period, warm-ups before training sessions and matches lasted 25–35 minutes. They included running drills randomly selected by the coach, alongside exercises for strength, balance, and plyometrics (skipping rope, high knees, lunges, squats, planks, and squat jumps). Sustained injuries were recorded during each training session or match in accordance with the FIFA Medical Assessment and Research Centre (F-MARC) consensus recommendations on injury data collection procedures in football [6].
The Incidence Rate (IR) was calculated as the number of injuries per 1000 player-hours of football exposure.
The Incidence Rate (IR) was calculated using the following formula:
IR = (N / ∑PD) x 1000,
where N is the number of injuries in the study group during the study period; ∑PD is the total player-hours of all training sessions/matches during the study period;
∑PD = P₁ x D₁ + P₂ x D₂ + … + Pₙ x Dₙ,
where P is the number of players participating in a single training session/match; D is the duration of a single training session/match in hours; n is the total number of training sessions/matches.
The overall incidence rate was calculated, alongside separate calculations for injury rates during training sessions (training injury rate) and during matches against other teams (match injury rate). Injury patterns were evaluated by anatomical location (corresponding to the injured body region) and by severity level. Severity was determined by the number of days the athlete was unable to fully train, starting from the day following the injury: Grade I — minimal (1–3 days); Grade II — mild (4–7 days); Grade III — moderate (8–28 days); Grade IV — severe (more than 28 days) [6].
Statistical Methods
Due to the small sample size, the non-parametric Wilcoxon signed-rank test for two related samples was used. Differences in incidence rates and the number of injuries by severity level during training sessions versus matches were determined. Changes in metrics were considered statistically significant at p < 0.05.
Results
During the study period, the total training/match time was 81 hours, which equated to 972 player-hours when adjusted for the number of players. The training period accounted for 576 player-hours, while matches accounted for 396 player-hours. The number and severity of injuries sustained during these periods are shown in Table 1.
Table 1
Distribution of Injuries by Anatomical Location and Severity
|
Location |
Overall Injury Rate |
Training Injury Rate |
Match Injury Rate | ||||||||||||
|
n |
Severity, grade |
n |
Severity, grade |
n |
Severity, grade | ||||||||||
|
I |
II |
III |
IV |
I |
II |
III |
IV |
I |
II |
III |
IV | ||||
|
Head |
1 |
0 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
0 |
1 |
0 |
0 |
|
Shoulder |
1 |
0 |
1 |
0 |
0 |
1 |
0 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
Forearm |
1 |
0 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
0 |
1 |
0 |
0 |
|
Hand |
2 |
0 |
1 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
2 |
0 |
1 |
1 |
0 |
|
Groin region |
4 |
0 |
2 |
2 |
0 |
1 |
0 |
1 |
0 |
0 |
3 |
0 |
1 |
2 |
0 |
|
Back |
1 |
0 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
0 |
1 |
0 |
0 |
|
Hamstring |
5 |
1 |
2 |
2 |
0 |
2 |
1 |
1 |
0 |
0 |
3 |
0 |
1 |
2 |
0 |
|
Anterior thigh |
2 |
0 |
1 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
2 |
0 |
1 |
1 |
0 |
|
Knee joint |
3 |
0 |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
0 |
2 |
0 |
1 |
0 |
1 |
|
Anterior lower leg |
4 |
0 |
2 |
2 |
0 |
0 |
0 |
0 |
0 |
0 |
4 |
0 |
2 |
2 |
0 |
|
Posterior lower leg |
2 |
0 |
1 |
1 |
0 |
1 |
0 |
1 |
0 |
0 |
1 |
0 |
0 |
1 |
0 |
|
Ankle joint |
3 |
0 |
1 |
1 |
1 |
1 |
0 |
1 |
0 |
0 |
2 |
0 |
0 |
0 |
1 |
|
Foot |
2 |
0 |
1 |
1 |
0 |
1 |
1 |
1 |
0 |
0 |
1 |
0 |
0 |
1 |
0 |
|
Total |
31 |
1 |
16 |
12 |
2 |
9 |
2 |
6 |
1 |
0 |
22 |
0 |
10 |
10 |
2 |
As shown in the presented data, the vast majority of injuries involved the lower extremities and the groin area. Specifically, the highest number of injuries was associated with the hamstrings (5 cases), groin ligaments and the anterior shin (4 cases each), and the knee and ankle joints (3 cases each). Moderate injuries accounted for half of all cases (51.6 %), while more than a third (38.7 %) were moderate injuries. Severe injuries were associated with ligament damage to the ankle and knee joints, accounting for 6.5 %. Minimal injuries occurred in 3.2 % of cases.
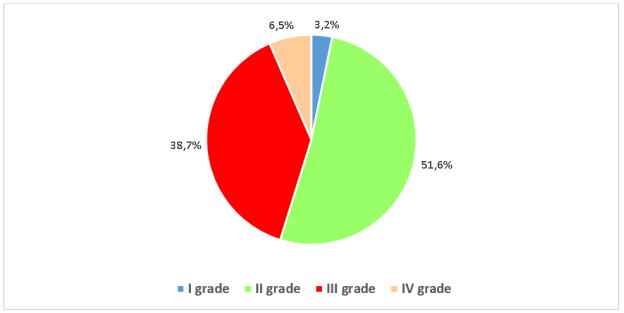
Fig. 1. Overall Injury Severity Distribution
The incidence rate differed significantly between the training and match periods. Injuries occurred nearly 3.5 times more frequently during matches against other teams than during training sessions (IR 55.5 and 15.6, respectively; p=0.002). The injury patterns by anatomical location showed no significant differences between the training and match periods. However, regarding severity, a significant difference was observed for moderate injuries—their proportion was 4 times higher during matches (45.5 % versus 11.1 %; p=0.006). A comparative analysis of overall incidence rates and injury severity levels during the training and match periods is presented in Table 2.
Table 2
Overall Incidence Rate and Severity
|
Incidence Rate |
Injury Severity Grade, n (%) | |||||
|
n |
IR |
I |
II |
III |
IV | |
|
Entire |
31 |
31,9 |
1 (3,2 %) |
16 (51,6 %) |
12 (38,7 %) |
2 (6,5 %) |
|
Training |
9 |
15,6 |
2 (22,2 %) |
6 (66,7 %) |
1 (11,1 %) |
0 |
|
Matches |
22 |
55,5 |
0 |
10 (45,5 %) |
10 (45,5 %) |
2 (9 %) |
|
Wilcoxon test, р |
0,002 * |
0.165 |
0.099 |
0.006 * |
0,082 | |
*Statistically significant (p < 0.05)
An analysis of the changes in injury patterns revealed that the increase in the proportion of moderate injuries during matches occurs due to a decrease in the share of minimal and mild injuries, which carry a greater relative weight during training sessions. Furthermore, severe injuries were identified exclusively during the match period.
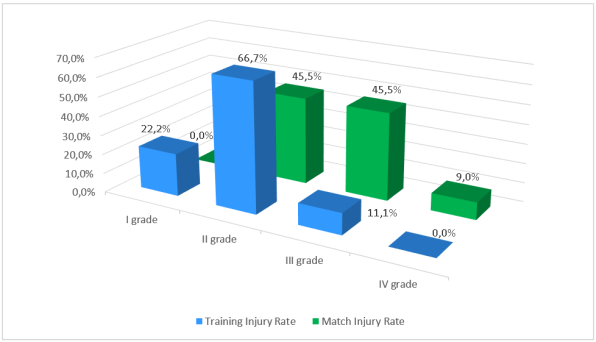
Fig. 2. Injury Severity Distribution During Training and Matches
Discussion
Overall incidence rate is an important characteristic of any sport [1–7]. At the same time, one of the primary objectives of sports medicine is to reduce the likelihood of sustaining injuries. To achieve this goal, it is crucial to understand the injury mechanisms, features, and injury patterns characteristic of each sport [7, 8]. We observed a relatively high incidence rate in the study group, which could be attributed to insufficient physical conditioning of the athletes and the «amateur» level of the matches. An analysis of the overall injury patterns demonstrated that the incidence of mild injuries was the highest, which aligns with findings from other researchers regarding non-professional players [8–10]. Moderate injuries ranked second, whereas the incidence of minimal and severe injuries was low. Similar findings were reported in a study by Marques C. et al., which also showed that a higher percentage of moderate and severe injuries is characteristic of non-professional players, whereas the severity of injuries decreases as the level of training improves [10]. The primary anatomical locations of injuries were the lower extremities and the groin area, which also coincides with literature data [1, 3-5, 8, 11]. Hamstring injuries held a leading position, which could be a consequence of inadequate conditioning of the hamstring muscles. Furthermore, severe injuries were exclusively associated with the joints of the lower extremity.
A comparative analysis of training and match-related injuries revealed specific patterns. First, the incidence rate was significantly higher during the match period. In addition, all severe injuries were sustained during matches against other teams. The redistribution of injuries by severity level in the match period compared to the training period occurred due to a decrease in the proportion of minimal and mild injuries and an increase in the share of moderate and severe injuries. This may reflect maximum emotional and physical exertion, as well as a decrease in body control and a greater number of potentially hazardous movements by the athletes [12-14]. Our findings are consistent with the results of several studies that have shown a higher incidence of injuries specifically during the match period [1, 10, 11].
Conclusion
In conclusion, amateur athletes aged 15–17 years are characterized by a relatively high overall incidence rate, with injuries predominantly occurring during the match period and affecting the lower extremities and groin area. The reasons for this specific injury incidence and pattern may include insufficient player expertise, a lack of body control skills, improper foot and shin placement, and inadequate conditioning of the hamstring muscles.
In this regard, injury prevention among young football players is of particular relevance, including the use of modern warm-up and training programs, one of which could be the «FIFA 11+» exercise complex.
References:
- Rozina MA, Radetskiy AYu, Mukharamova AM, Koroleva IuA, Shesternina VS, Semenov AN, Emelianov DS, Davydov DD, Kuznetsova OD. Injuries among young male and female footballers training at the academy. Medicine: Theory and Practice. 2025;10(1):7–15. (In Russian). DOI: https://doi.org/10.56871/MTP.2025.82.51.001
- Bayt D. R., Bell T. M. Trends in paediatric sports-related injuries presenting to US emergency departments, 2001–2013. Inj. Prev. 2016;22:361–364. doi: 10.1136/injuryprev-2015–041757.
- López-Valenciano A., Ruiz-Pérez I., Garcia-Gómez A., Ve ra-Garcia F. J., De Ste Croix M., Myer G. D., Ayala F. Epidemiology of injuries in professional football: a systematic review and meta-analysis. Br J Sports Med. 2020;54(12):711 718. DOI: 10.1136/bjsports-2018–099577.
- Al’-Dzhaberi A. S., Rapoport L. A. Sports injuries in football according to the age of players. Izvestija Tul’skogo gosudarst vennogo universiteta. Fizicheskaja kul’tura. Sport. 2022;8:58 63. (In Russian). DOI: 10.24412/2305–8404–2022–8–58–63.
- Mazur A. I. Epidemiology of sports injuries in the aspect of medical rehabilitation. Medicinskie novosti. 2012;11:46–50. (In Russian).
- Fuller C. W., Ekstrand J., Junge A., Andersen T. E., Bahr R., Dvorak J., Hägglund M., McCrory P., Meeu wisse W. H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med. 2006;40(3):193–201. DOI: 10.1136/bjsm.2005.025270.
- Savchenko I. V., Avtomonova T. S., Martinen M. S. Features of traumatic injuries in children and the factors that determine them (literature review). Medicine: Theory and Practice. 2021;6(2):46–53. (In Russian).
- Faude O., Rößler R., Junge A. Football injuries in children and adolescent players: Are there clues for prevention? Sports Med. 2013;43:819–837. doi: 10.1007/s40279–013–0061-x.
- Bangsbo J., Hansen P. R., Dvorak J., Krustrup P. Recreational football for disease prevention and treatment in untrained men: A narrative review examining cardiovascular health, lipid profile, body composition, muscle strength and functional capacity. Br. J. Sports Med. 2015;49:568–576. doi: 10.1136/bjsports-2015–094781.
- Marques C, Rebelo M, Crisóstomo R, Honório S, Duarte-Mendes P, Petrica J and Serrano J Descriptive analysis of injury types and incidence during futsal preseason across different competitive levels. Front. Sports Act. Living 6(2024):1363006. doi: 10.3389/fspor.2024.1363006.
- Robles-Palazón F. J., López-Valenciano A., De Ste Croix M., Oliver J. L., García-Gómez A., Sainz de Ba randa P., Ayala F. Epidemiology of injuries in male and female youth football players: A systematic review and meta-analysis. J Sport Health Sci. 2022;11(6):681–695. DOI: 10.1016/j.jshs.2021.10.002.
- GabbettTJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. (2016) 50(5):273–80. 10.1136/bjsports-2015–095788.
- Dvorák J. Give Hippocrates a jersey: Promoting health through football/sport. Br. J. Sports Med. 2009;43:317–322. doi: 10.1136/bjsm.2009.059618.
- Jinfeng Yang, Yang Wang, Jianxin Chen, Jinqi Yang, Na Li, Chun Wang, Yuanpeng Liao. Effects of the “FIFA11+ Kids” Program on Injury Prevention in Children: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2022 Sep 23;19(19):12044. doi: 10.3390/ijerph191912044.

