In the Kyrgyz Republic the epidemiological situation in TB remains rather tense. In Bishkek for a long period (1993–1998 and 2003–2013) the TB incidence exceeded the national level, including among the child population. The tuberculosis prevalence is analyzed by social and ethnic groups in the city Bishkek.
Tuberculosis is a socially important disease which by the current world statistics is showing a tendency to spread further. Annually 8–10 mil. people get ill with tuberculosis and about 3 mil. people die from it [1;3;5;8;10;11].
The current tuberculosis epidemiological situation has become more acute in all countries of the world. While there is a fall in the incidence of tuberculosis, more younger age cases occur, and what is most concerning, the next epidemiological surge is forming, of a new quality, characterized by high levels of destructive and complicated forms of pulmonary tuberculosis, intensive development of a reservoir of drug resistant mycobacteria, a high level of reactivation of tuberculosis after cure [2;4;6;7;9;12].
Based on the tuberculosis situation the Government of the Kyrgyz Republic adopts strategic plans to improve the epidemiological situation in tuberculosis in the country. The new strategy of the health sector “Den-Sooluk” and the National Programme “Tuberculosis-IV” was confirmed by the Decree of the Government of the Kyrgyz Republic of 10 June 2013 No.325 for the years 2013–2016 as well as in accordance with the Law of the Kyrgyz Republic “On protection of health of the population from tuberculosis”.
The aim of the study was to carry out comparisons in the epidemiological situation regarding tuberculosis in the city Bishkek and Kyrgyz Republic.
Materials and methods
Statistical data from the Republican Medical Information Centre, the National Phthisiology Centre, the City Tuberculosis Hospital, the City Children’s Tuberculosis Hospital and the City Centre for Tuberculosis Control were used for medico-demographical, sanitary-epidemiological analyses taking into consideration WHO guidelines. 3700 case histories were handled.
Results
In the Kyrgyz Republic the epidemiological situation in tuberculosis is heightened. The annual average number of new tuberculosis cases over the years 1993–2013 was 5938±338, being an average of 116.97±6.5 per 100 000 population in this period. The tuberculosis epidemiological peak falls on the year 2001–167.8 cases per 100 000 population. By 2011 the incidence decreased to 100.4 per 100 000 population. In 2012 there begins a new rise in the incidence which amounted to 102.4 in 2013.
As can be seen in fig.1, in 2001 it was managed to stop a growth in tuberculosis but it failed to reach the initial level despite an active implementation of DOTS strategy in all primary health care organizations.
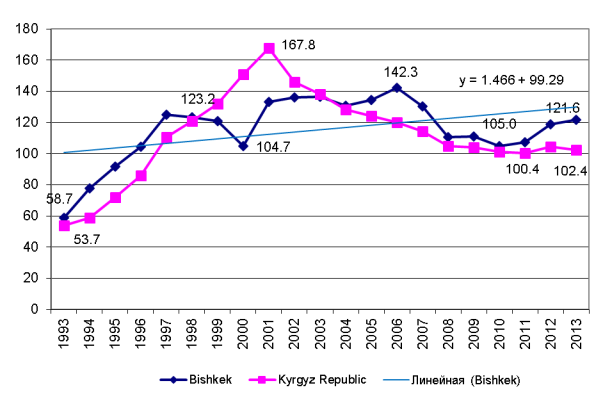
Fig.1. Tuberculosis trends in the city Bishkek and the Kyrgyz Republic over the years 1993–2013 (per 100 000 population)
The tuberculosis epidemiological situation is regarded as normal if the incidence is less than 30.0 per 100 000 population. Because the world experience shows that if quality prevention measures are implemented this level of incidence can be achieved at least. An increase and a decrease in the population morbidity of tuberculosis is one of the main indicators of infection spread and a sign of unfavorable epidemiological situation.
Tuberculosis morbidity of inhabitants of the city Bishkek has its own distinctive features. Two epidemiological peaks were observed: in 1997–123.2 and in 2006–142.3 per 100 000 population, the interval between them being 9 years. In Bishkek the incidence of tuberculosis was above the national rate for a long period of time (1993–1998 и 2003–2013) except for the period of the highest epidemic rise in the incidence in the country as a whole (1999–2002). Possibly the population of the capital is a major reservoir keeping tuberculosis infection in the inter-epidemic period. So, increasing preventive activity at the population of Bishkek could decrease tuberculosis morbidity in the country as a whole.
According to data from the Republican Medical Information Centre, which records new cases of tuberculosis, new cases of pulmonary tuberculosis make up 74.2±3.1 % whereas extrapulmonary cases make up 25.8±2.9 %, i.e. 3 times less. According to 2013 data, among new cases of tuberculosis, the rate of pulmonary tuberculosis was 67.7 % and that of extrapulmonary tuberculosis — 32.3 %.
Distribution of patients with newly diagnosed tuberculosis by gender is shown in table 1. Among patients with tuberculosis, males are predominant. The proportion of males was 54.9 % in the tuberculosis ill group and 46.4 % in population. In the tuberculosis group, there were on average 1242 males per 1000 females, whereas 867 in population. By this parameter, in the tuberculosis group, the predominance of males was 42 %.
It follows from this that predisposition to tuberculosis is 1.4 times higher in men than in women. The average age of persons newly ill with tuberculosis was 37±0.6 years.
Table 1
Cases of tuberculosis by gender in the population of the city Bishkek
|
Years |
Number |
Proportion of males in a group |
Males per 1000 females |
Cases per 100000 |
Significance | |||||||
|
males |
females | |||||||||||
|
M |
F |
pati-ents |
popu-lation |
pati-ents |
popu-lation |
P |
m |
P |
m |
t |
P | |
|
2009 |
524 |
407 |
56.3 |
46.4 |
1287 |
865 |
134.5 |
5.8 |
90.4 |
4.4 |
6.1 |
< 0.001 |
|
2010 |
476 |
420 |
53.1 |
46.3 |
1133 |
866 |
118.9 |
5.4 |
90.9 |
4.4 |
4.0 |
< 0.001 |
|
2011 |
511 |
418 |
55.0 |
46.4 |
1231 |
867 |
127.7 |
5.6 |
90.5 |
4.4 |
5.2 |
< 0.001 |
|
2012 |
591 |
461 |
56.2 |
46.5 |
1282 |
869 |
143.4 |
6 |
97.4 |
4.6 |
6.1 |
< 0.001 |
|
2013 |
364 |
310 |
54.0 |
46.4 |
1279 |
867 |
132.1 |
5.7 |
92.3 |
4.5 |
5.4 |
< 0.001 |
|
Average |
493 |
403 |
54.92 |
46.4 |
1242 |
866.8 |
131.3 |
5.7 |
92.3 |
4.46 |
5.36 |
< 0,001 |
Among children ill with tuberculosis cases of extrapulmonary tuberculosis are significantly predominant — 47.9 per 100 000 population (table 2). The younger the age group, the higher proportion of extrapulmonary tuberculosis: 0–4 years — 79.1 %; 5–6 years — 87.1 %; 7–14 years — 69.4 %.
Together with the high adult tuberculosis morbidity, a high morbidity is observed in children including both cases of complicated primary tuberculosis and cases with the induration stage process indicating late diagnosis of tuberculosis.
Table 2
Distribution of newly diagnosed cases of tuberculosis in children, city Bishkek
|
Form of tuberculosis |
Total |
Including in the age | ||||||
|
0–4 years |
5–6 years |
7–14 years | ||||||
|
n |
per 100 000 |
n |
per 100 000 |
n |
per 100 000 |
n |
per 100 000 | |
|
Total |
348 |
57.8 |
86 |
37.5 |
62 |
78.9 |
337 |
114.6 |
|
Pulmonary |
49 |
8.1 |
13 |
5.7 |
8 |
10.2 |
103 |
35.0 |
|
Extrapulmonary |
288 |
47.9 |
68 |
29.6 |
54 |
68.7 |
234 |
79.6 |
The statistical evidence indicates an exogenous nature of tuberculosis in children, who get infected from adults in tuberculosis infection foci. In the Kyrgyz Republic, on average, there are 72 excreters per 100 000 population. 2.2–2.4 healthy persons get infected per each one of them.
Our analysis of the impact of vaccination on the epidemic process of tuberculosis revealed the following. In the period between 2009 and 2011 200676 children were immunized, tuberculosis was diagnosed in 106 of them (0.05 %). The incidence rate was 52.8 per 100 000 pediatric population. By numeric data, on average, 0.05 % of vaccinated children lost or did not acquire post-vaccinal immunity, which is in agreement with reports of other authors stating that tuberculosis vaccination does not provide a complete prevention of tuberculosis [3, 5].
The analysis of the incidence of tuberculosis by social population groups showed that 1132 patients were admitted to the Bishkek city Tuberculosis Hospital in 2011, of them 849 (75.0 %) were Kyrgyz, 183 (16.2 %) — Russians. The rest — 100 patients (8.8 %) were other ethnic groups (table 3).
The ethnic composition of tuberculosis patients reflects the ethnic composition of the population of the city Bishkek.
First place is occupied by the homeless, i.e. persons who have no work and no fixed abode. Their proportion is 8.9 %. Second to them are students follow, with a proportion of 6.1 %. The 3rd rank is shared by pensioners, 4.8 %, and disabled persons, 4.2 %. The hospitalized population includes rather a large group of prisoners, 2.6 %, and military personnel, 1.5 %. Other patients have a proportion less than 1 %. A low proportion of the working class, 0.9 %, is of notice, while in the total number of patients with tuberculosis, working age persons make up 77.6 %. This discrepancy is explained by that the working age population prefers ambulatory treatment as it allows them to work and stay on relief.
Thus, any person can acquire tuberculosis, at any age. The homeless group presents a scientific interest, it is a population group without job and without fixed abode. 216 case histories of tuberculosis were selected by continuous sampling. In Bishkek in 2009–2011 a total of 346 homeless persons ill with tuberculosis was recorded. They were found mostly by phthisiatricians making household-to-household rounds, ambulance teams, policemen and only 23 % sought medical attention themselves. Of the total number of homeless persons, 195 (56.45 %) were newly ill with tuberculosis, 112 (32.4 %) had a relapse and no information on 39 (11.3 %) (table 4).
Table 3
Incidence of tuberculosis by ethnic groups, Bishkek, 2009–2011
|
Ethnic groups |
2009 |
2010 |
2011 | |||||||||
|
Popula-tion |
Number of patients |
Per 100 000 popula-tion |
% |
Popula-tion |
Number of patients |
Per 100 000 popula-tion |
% |
Popula-tion |
Number of patients |
Per 100 000 popula-tion |
% | |
|
Kyrgyz |
567797 |
785 |
92.7 |
72.2 |
586864 |
728 |
84.7 |
66.0 |
606917 |
849 |
97.1 |
75.0 |
|
Russians |
188105 |
192 |
22.7 |
17.7 |
182897 |
222 |
25.8 |
20.0 |
177757 |
183 |
20.9 |
16.2 |
|
Ukrainians |
7527 |
45 |
5.9 |
4.1 |
7083 |
24 |
2.8 |
2.2 |
6530 |
12 |
1.4 |
1.1 |
|
Uzbeks |
11969 |
25 |
3.0 |
2.3 |
12129 |
87 |
10.1 |
7.8 |
12284 |
46 |
5.3 |
4.1 |
|
Koreans |
12094 |
11 |
1.3 |
1.0 |
11886 |
9 |
0.9 |
0.8 |
11808 |
8 |
0.9 |
0.7 |
|
Uigurs |
13583 |
- |
- |
- |
13788 |
- |
- |
- |
13944 |
- |
- |
- |
|
Tatars |
12524 |
6 |
0.7 |
0.6 |
12266 |
10 |
1.2 |
0.9 |
11996 |
16 |
1.8 |
1.4 |
|
Kazakh |
9019 |
6 |
.07 |
0.6 |
8989 |
- |
- |
- |
9089 |
4 |
0.4 |
0.3 |
|
Dungans |
4127 |
- |
- |
- |
4331 |
1 |
0.1 |
0.1 |
4364 |
1 |
0.1 |
0.1 |
|
Turks |
3203 |
1 |
0.11 |
0.11 |
3264 |
4 |
0.5 |
0.3 |
3305 |
4 |
0.4 |
0.3 |
|
Germans |
2569 |
6 |
0.7 |
0.6 |
2576 |
7 |
0.8 |
0.6 |
2498 |
3 |
0.3 |
0.3 |
|
Tajiks |
833 |
- |
- |
- |
854 |
- |
- |
- |
871 |
- |
- |
- |
|
Other |
13117 |
10 |
1.2 |
0.08 |
12866 |
18 |
2.1 |
1.6 |
12994 |
6 |
0.7 |
0.5 |
|
Total |
846467 |
1087 |
128.4 |
100.0 |
859795 |
1103 |
128.3 |
100.0 |
874357 |
1132 |
129.5 |
100.0 |
Table 4
Distribution of homeless persons ill with tuberculosis by the primary and relapse group
|
Patient group |
Recorded total |
Included those recorded in | |||||
|
the in-patient hospital |
the dispesary | ||||||
|
n |
% |
Per 100 000 |
n |
% |
n |
% | |
|
New cases |
195 |
56.4 |
7.5 |
110 |
50.9 |
85 |
65.4 |
|
Relapses |
112 |
32.4 |
4.3 |
106 |
49.1 |
6 |
4.6 |
|
Unknown |
39 |
11.3 |
1.5 |
0 |
0.0 |
39 |
30.0 |
|
Total |
346 |
100.0 |
13.3 |
216 |
100 |
130 |
100 |
The incidence of tuberculosis per 100 000 population increases by 13.3 persons annually due to the homeless portion. Moreover, relapses among the homeless group occur more frequently than in general: at the ratio of 1: 2 (112 relapses for 195 new cases). In the city Bishkek an increase in the incidence due to relapse of tuberculosis in homeless persons is an average of 4.3 units, with males predominating (67.7 %) over females (32.3 %) (table 5). Homeless patients under age 30 years make up 28.5 %, while this figure is 52.3 % for the general adult sample. The proportion of patients of higher than 30 years of age is 71.5 % for the homeless, while it is 47.7 % for the general patient population. It can be concluded that homeless persons fall ill with tuberculosis at a greater age. This is supported by the average age of homeless persons with tuberculosis being 40.8±0.6 years versus 36.2±1.3 in the general sample. A difference of 4.6 years is statistically significant.
Table 5
Distribution of homeless persons ill with tuberculosis by the gender and age
|
Age group |
Number, by fact |
Number, after smoothing | ||||||||
|
Total |
including |
Total |
including | |||||||
|
M |
F |
M |
F | |||||||
|
n |
% |
n |
% |
n |
% | |||||
|
Under 19 |
21 |
11 |
10 |
|
|
|
|
|
| |
|
20–24 |
11 |
3 |
8 |
18 |
5.1 |
16 |
6.9 |
10 |
8.6 | |
|
25–29 |
40 |
32 |
8 |
20 |
5.7 |
19 |
8.1 |
9 |
7.8 | |
|
30–34 |
27 |
19 |
8 |
31 |
9.1 |
24 |
10.2 |
14 |
12.9 | |
|
35–39 |
40 |
16 |
24 |
61 |
17.5 |
32 |
13.8 |
23 |
20.7 | |
|
40–44 |
88 |
56 |
32 |
69 |
19.9 |
40 |
17.1 |
23 |
20.7 | |
|
45–49 |
48 |
40 |
8 |
63 |
18.1 |
41 |
17.5 |
16 |
14.6 | |
|
50–54 |
24 |
19 |
5 |
38 |
10.9 |
27 |
11.4 |
8 |
6.9 | |
|
55–59 |
24 |
16 |
8 |
28 |
8.2 |
21 |
8.9 |
6 |
5.2 | |
|
60+ |
24 |
24 |
0 |
19 |
5.4 |
14 |
6.1 |
3 |
2.6 | |
|
Total |
346 |
234 |
112 |
346 |
100 |
234 |
100.0 |
112 |
100.0 | |
The level of probability significance is P<0.01. In the total number of homeless persons the proportion of working age persons is 76.9 % while it is known that tuberculosis occurs most frequently in young people [7].
Thus, socially vulnerable persons (the homeless) have a high level of predisposition to pulmonary tuberculosis morbidity. They have the lowest rates of clinical cure, closure of destructive process cavities, removal from being on the monitoring list because they practically do not stop being smear positive, and they also have high rates of early and late relapses. The severity and clinical features of tuberculosis in the homeless are mostly due to their unorganized state and inclination to vagrancy. The homeless cohort is a reservoir of infection, contributing to tuberculosis incidence, prevalence and mortality.
In the Kyrgyz Republic annually 500 to 662 persons die from tuberculosis. In the period from 2001 to 2013 tuberculosis mortality decreased from 23.6 to 8.1 cases per 100 000 population. It also should be pointed out that through the period from 1993 to 2013 mortality from tuberculosis in Bishkek was higher than the national level and more than twice as high during the epidemic peaks (fig.2).
Beginning in 2000 in Bishkek there is observed a decreasing tendency for tuberculosis mortality, it is connected not only with decreasing morbidity but also with implementation of more effective therapy methods.
Thus, the mortality levels of the population due to tuberculosis indicate a difficult epidemiological situation of tuberculosis. The reasons for high levels of tuberculosis lethality are late diagnosis and late hospitalization of sick persons which leads to severe and complicated forms of tuberculosis ending frequently in a fatal outcome.
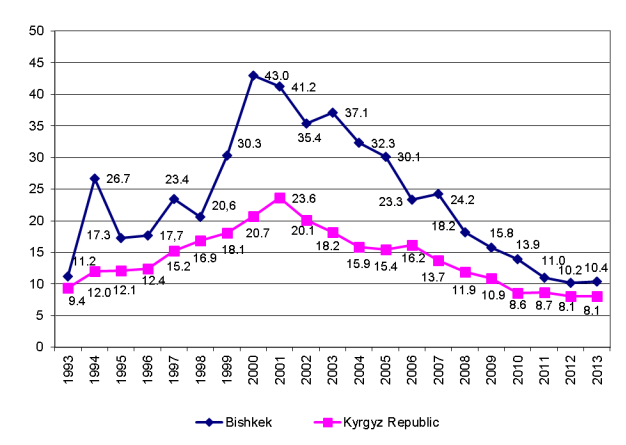
Fig. 2. Tuberculosis mortality trend in the city Bishkek and the Kyrgyz Republic over the years 1993–2013 (per 100 000)
Conclusions
The epidemiological situation of tuberculosis in Kyrgyzstan as a whole remains tense. The worsening welfare standards of the population, the increasing number of unemployed and persons without fixed abode, intensification of migration processes, instable economic situation, decreasing effectiveness of therapeutic and preventive measures, insufficient finance of antituberculosis measures, all this contributes to the high prevalence of tuberculosis where almost half of cases have a pulmonary form and are even excreting the microorganism.
References:
- Bogorodskaya E. M. Quitting treatment is the main reason for low effectiveness of treatment of tuberculosis patients In: Organization of therapeutic service to persons ill with tuberculosis: Proceedings of the Conference of Chief Physicians and Managers of Organizational-and-Methodical Departments of Tuberculosis Institutions (1–2 July, 2008), Research Institute of Phthisiopulmonology of the I. M. SEchenov Moscow Medical Academy, chief editor M. I. Perelman. Moscow, 2008, p.45–50. (Russian)
- Bubochkin B. P., Zasukhin O. A. The present-day risk factors and specific features of tuberculosis detection in young persons. Problemy tuberkuleza (Problems of Tuberculosis), 1988, (11):5–8. (Russian)
- Geodakyan V. A. Gender differential mortality and the norm of reaction. Biologicheskii zhurnal Armenii (Biological Journal of Armenia), 26(6):3–11.
- Zakirova K. A. The modern epidemiologicalal situation and organizational aspects of improving tuberculosis prevention. PhD thesis, Moscow, 2012, 273 p. (Russian)
- Ilyina T.Ya., Muminov T. A., Kaldibaev S. K. Respiratory tuberculosis and treatment effectiveness in some high risk groups. Problemy tuberkuleza (Problems of Tuberculosis), 2000, (4):9–11. (Russian)
- Muminov T. A., Rakisheva A. S. Tuberculosis in penal institutions. Almaty, 2002, 535 p. (Russian)
- Fedorova S. V. Development and realization of new approaches to tuberculosis prevention work targeted at higher school students in the city Bishkek. Candidate’s thesis, Bishkek, 2008, 174 p. (Russian)
- Finkel E. A., Alisherov A.Sh., Mikhailova L. V. Bacteriological diagnosis of tuberculosis, Bishkek: Ilim, 1998, 248 p. (Russian)
- Apti G., Dantes E. The clinical-radiological profile of pulmonary tuberculosis in a young woman from community with a high burden of disease. Europ. Resp. J., 2004, 28, Suppl.48, p.443.
- Global tuberculosis control: surveillance, planning, financing. Rep. World Health Organ, Geneva, 2009, 180 p.
- Holmes C. B., Hausler H., Nunn P. A review of sex differences in the epidemiology of tuberculosis. Int. J. Tuberc. Lung Dis., 1998, 2(2):96–104.
- Itah A. Y., Udofia S. M. Epidemiology and endemicity of pulmonary tuberculosis (PTB) in Southeastern Nigeria. Southeast Asian J. Trop. Med. Public Health, 2005, 36(2):317–323.

